The Cortisol Reset Protocol
The complete protocol for the cortisol type — stress recovery practices that actually work, sleep architecture, and the full toolkit for getting out of chronic alarm mode.
Learn MoreWhen the body cannot tell the difference between a deadline and a tiger
You wake up tired but still wired. The afternoon comes and you cannot relax. By night you are exhausted but cannot quite fall asleep, and when you do, you are awake again at 3 AM. Around the middle of your body, weight has settled in a place it never did before. There is a name for this pattern.
The High Cortisol Type is the third of the five hormonal patterns identified in the Hormetics framework, co-developed by health researcher Elwin Robinson and Dr. Miriam Mikicki MD, an IFM-certified functional medicine physician.
If the following picture is recognizable, this pattern may be in play:
These patterns are characteristic of a chronically activated stress response, sustained over months and years ¹.
Cortisol is a steroid hormone produced by the adrenal glands, two small organs that sit on top of the kidneys ². It is the body's primary glucocorticoid and one of the central hormones of the stress response.
Cortisol is not, in itself, a problem hormone. The body needs it. It mobilizes glucose for energy, modulates inflammation, regulates blood pressure, supports immune function, and helps drive the daily rhythm of waking and sleeping ³. A healthy cortisol curve rises sharply in the first half hour after waking (called the cortisol awakening response), gradually declines through the day, and reaches its lowest point in the early hours of the night ⁴.
The system is designed for short, intense stressors followed by recovery. A burst of cortisol for the duration of the threat, then a return to baseline. The hormone evolved in a context where stress was acute (a physical danger, a social conflict) and where the rest of the day allowed recovery ⁵.
This is what cortisol is supposed to do.
High Cortisol is what happens when the stress response, designed for short bursts, becomes a sustained pattern. The HPA axis (hypothalamic-pituitary-adrenal axis), which controls cortisol release, gets stuck in an elevated state ⁶. The body does not return to baseline. Recovery does not happen. And cortisol, helpful in the short term, becomes destructive over time.
The downstream effects of chronic elevation are well documented:
The pattern is sometimes called ‘adrenal fatigue’ in popular health writing, though that specific framing is contested in the endocrinology literature ¹⁴. The phenomenon itself (the dysregulated HPA axis under chronic stress) is well established. The terminology has shifted toward ‘HPA axis dysfunction’ in clinical settings.
High Cortisol is rarely about one stressful event. It develops through accumulated, sustained activation over months and years.
Chronic psychological stress. Work pressure, relationship strain, financial worry, caregiving demands, prolonged uncertainty. The brain does not distinguish well between these and physical threats ¹⁵.
Sleep deprivation. Inadequate or fragmented sleep directly elevates cortisol the following day ¹⁶. This is one of the most common entry points into the pattern.
Inflammatory load. Chronic inflammation, from any source, elevates cortisol as part of the body's compensatory response ¹⁷. Foods, environmental exposures, gut dysbiosis, and chronic infections can all contribute.
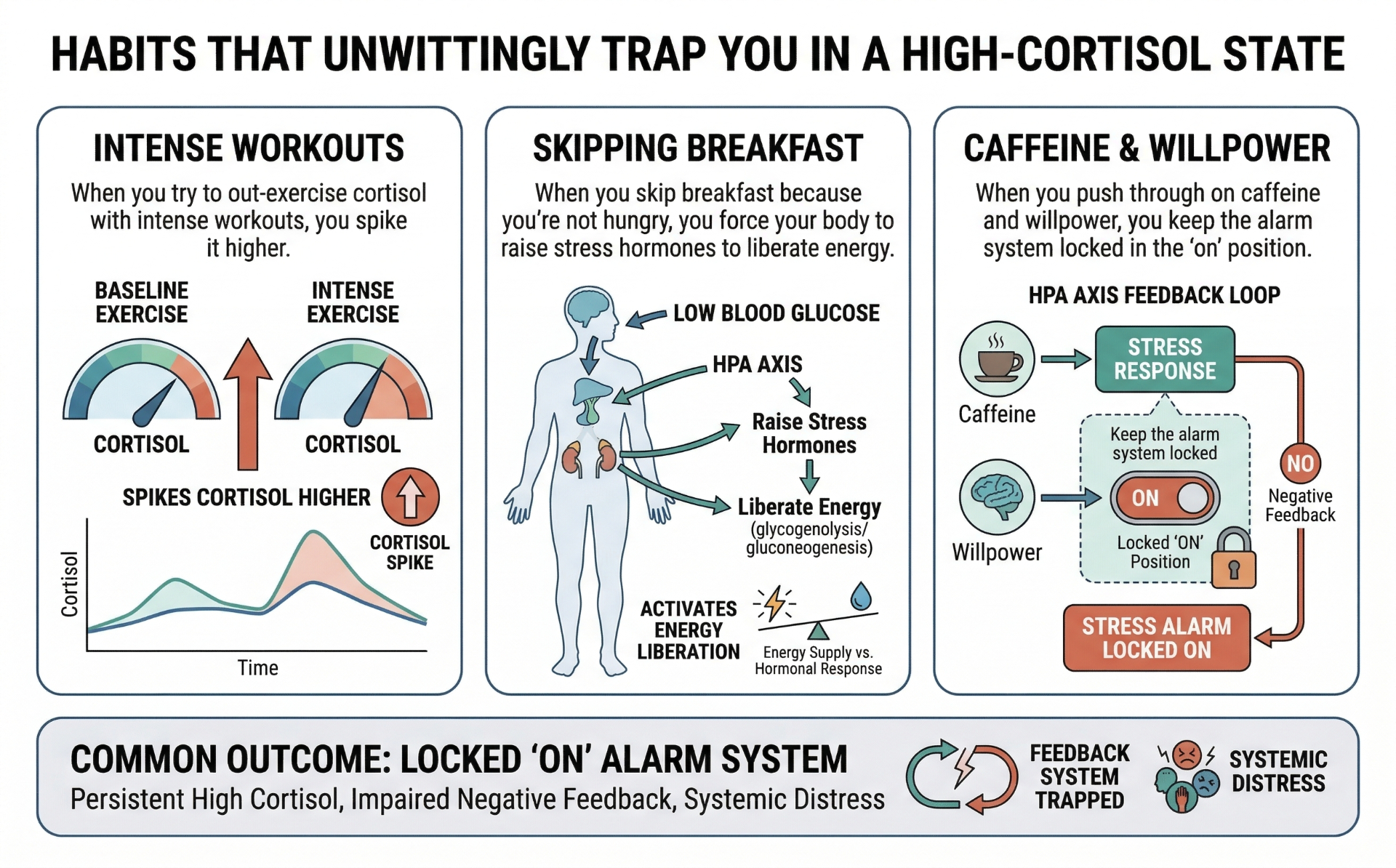
Caffeine and stimulant use. Regular caffeine consumption, especially in the afternoon, prolongs cortisol elevation. The half-life of caffeine is roughly 5 to 6 hours, but its effect on cortisol can persist longer ¹⁸.
Overtraining. Excessive high-intensity exercise without adequate recovery is a potent driver of HPA dysregulation ¹⁹.
Blood sugar instability. Skipping meals, fasting too aggressively, or eating only refined carbohydrates triggers cortisol release as a counter-regulatory hormone ²⁰.
Hypervigilance and trauma history. Past trauma, even decades old, can leave the nervous system primed for threat detection in a way that keeps cortisol chronically elevated ²¹.
The defining feature of the High Cortisol pattern is its self-reinforcing structure. Cortisol disrupts sleep, which raises cortisol. Cortisol promotes belly fat, which produces inflammatory cytokines, which raise cortisol. Cortisol blunts thyroid conversion, which slows metabolism, which makes weight harder to manage, which adds psychological stress, which raises cortisol ²².
The result is a pattern that does not simply resolve when the original stressor passes. Often the original stressor (the demanding job, the difficult relationship) is no longer the same, but the dysregulated HPA pattern remains. The nervous system has learned a setpoint. It does not unlearn quickly.
This is why people with this pattern often report that they cannot relax even when they finally have time to. The body has lost the off switch.

The standard advice for stress is ‘manage your stress better.’ This advice is not wrong, but it tends to focus on cognitive techniques (meditation, mindset, reframing) without addressing the physiological infrastructure of the stress response.
For someone with established High Cortisol, willpower-based stress management often underperforms because the underlying signaling is dysregulated. Meditation can help, but its effect is significantly amplified when it is layered on top of foundational corrections (sleep, light, blood sugar, inflammation). Without those foundations, the nervous system stays activated despite the practice.
Standard sleep advice also tends to underperform with this pattern. ‘Get eight hours’ is a useful goal, but if cortisol is dysregulated, sleep architecture is fragmented even when total time in bed is adequate ²³.
Pharmaceutical approaches (sleep aids, anxiolytics, antidepressants) can help with symptoms but do not directly correct the HPA axis dysfunction. In some cases they may inadvertently reinforce it ²⁴.
The deeper limitation of conventional approaches is that they tend to treat the symptoms of cortisol dominance (poor sleep, anxiety, weight gain) as separate problems rather than as expressions of a single dysregulated system.
The High Cortisol framework starts from a different premise: the goal is not to fight the stress response but to give the body the conditions in which the stress response can naturally complete and reset.
This is what the Hormetics system addresses for this type. The Cortisol Reset Protocol, co-developed by Elwin Robinson and Dr. Miriam Mikicki MD, works through the structural drivers of HPA dysregulation in a specific order. The details of the protocol are beyond the scope of this page, but the framework addresses sleep architecture, light exposure, blood sugar stability, nervous system regulation practices, and targeted nutritional and adaptogenic support. The approach is not ‘do more meditation.’ It is ‘give the system the inputs it needs to recalibrate.’
The first step is identifying which of the five Hormetics types applies to your specific situation.
High Cortisol rarely operates in isolation. Chronic cortisol elevation drives insulin resistance ²⁵ and contributes to leptin resistance through the inflammatory pathways that affect both ²⁶. It can also worsen estrogen dominance by interfering with hepatic detoxification ²⁷ and reduces metabolic rate by inhibiting active thyroid hormone ²⁸.
In Dr. Mikicki's clinical work with patients whose body composition does not respond to sound nutrition and exercise, cortisol is consistently among the first patterns she investigates. As she has put it: ‘I definitely see a link with cortisol and weight issues.’
If the description on this page sounds like your experience, the next step is the assessment.
Already taken the assessment and know you're a Cortisol Type? If so, the following could help:
The complete protocol for the cortisol type — stress recovery practices that actually work, sleep architecture, and the full toolkit for getting out of chronic alarm mode.
Learn More
Formulated to support healthy stress response and adrenal function.†
Learn MoreImportant: The Hormetics framework is an educational system designed to support hormonal and metabolic optimization. It is not a substitute for medical evaluation, diagnosis, or treatment. If you have a medical condition, are taking medication, or have specific health concerns, consult with your healthcare provider before making changes. Individual results vary.
We use cookies to ensure the best experience and for ad performance.