The Estrogen Reset Protocol
What to eat, what to avoid, the supplements that support the pattern, and the daily rhythms that move the needle on healthy estrogen metabolism.
Learn MoreWhen the issue is not how much, but how the body clears it
In women: weight that settles in the hips and thighs no matter what changes. Heavy cycles. Bloating that worsens before periods. Mood shifts that follow a predictable rhythm. In men: stubborn weight at the chest and waist, lower drive, a sense that the masculine balance has shifted. There is a hormonal explanation that connects all of these.
The High Estrogen Type is the fourth of the five hormonal patterns in the Hormetics framework, co-developed by health researcher Elwin Robinson and Dr. Miriam Mikicki MD, an IFM-certified functional medicine physician.
In women, common features of this pattern include:
In men, the pattern presents differently:
What links these very different presentations is not necessarily a high estrogen exposure, but a relative excess of estrogen activity, often combined with impaired clearance, compared to the other hormones the body uses to balance it ¹.
Estrogen is not a single hormone but a family of three: estradiol (E2, the most potent), estrone (E1), and estriol (E3) ². These are produced primarily by the ovaries in women and in smaller amounts by the testes and adrenal glands in men. Notably, fat tissue (adipose tissue) also produces estrogen in both sexes through the action of an enzyme called aromatase ³.
Estrogens regulate dozens of physiological processes: reproductive function, bone density, cardiovascular health, cognitive function, skin and tissue integrity, mood, fat distribution, and more ⁴. The hormones themselves are essential.
The body uses several mechanisms to keep estrogen activity in balance. One is direct opposition: progesterone, the other major female hormone, balances many of estrogen's effects on tissue growth and fluid retention ⁵. Another is clearance: the liver and gut work together to deactivate estrogen and remove it from the body so that levels stay within a healthy range ⁶.
When either of those mechanisms falters, the body drifts toward what is called estrogen dominance, even if absolute estrogen levels are not particularly high.
Most discussion of estrogen dominance focuses on production. The more common driver, in clinical observation, is impaired clearance.
The liver processes estrogen in two main phases ⁷:
Phase 1. A family of enzymes (the cytochrome P450 system, including CYP1A1, CYP1B1, and CYP3A4) converts estrogen into intermediate metabolites. Some of these metabolites (particularly the 2-hydroxyestrone pathway) are relatively benign. Others (the 4-hydroxyestrone pathway) are more reactive and require careful processing ⁸.
Phase 2. The intermediates from Phase 1 are conjugated (attached to other molecules) so they can be excreted. The two main pathways are methylation (requiring methyl donors and B vitamins) and glucuronidation (requiring intact liver function and balanced gut bacteria) ⁹.
If Phase 2 is bottlenecked (insufficient methylation cofactors, impaired glucuronidation, gut dysbiosis), the intermediate metabolites can recirculate, accumulate, and cause downstream effects ¹⁰.
The gut adds another layer. After estrogen is conjugated in the liver and excreted into the bile, it travels into the intestines for elimination. Certain gut bacteria produce an enzyme called beta-glucuronidase, which can deconjugate the estrogen and allow it to be reabsorbed back into circulation. The collection of estrogen-modulating gut bacteria is called the estrobolome ¹¹. When the estrobolome is dysbiotic (often through antibiotic exposure, processed diet, or chronic inflammation), estrogen recirculates rather than leaving the body.
There is one more layer specific to body composition. Aromatase, the enzyme in fat tissue that converts androgens to estrogen, is upregulated in conditions of inflammation, insulin resistance, and increased adiposity ¹². This creates the feedback loop that Elwin describes: more fat tissue produces more estrogen, more estrogen drives more fat storage in estrogen-sensitive areas, and the pattern reinforces itself.
Several specific drivers contribute to estrogen dominance.
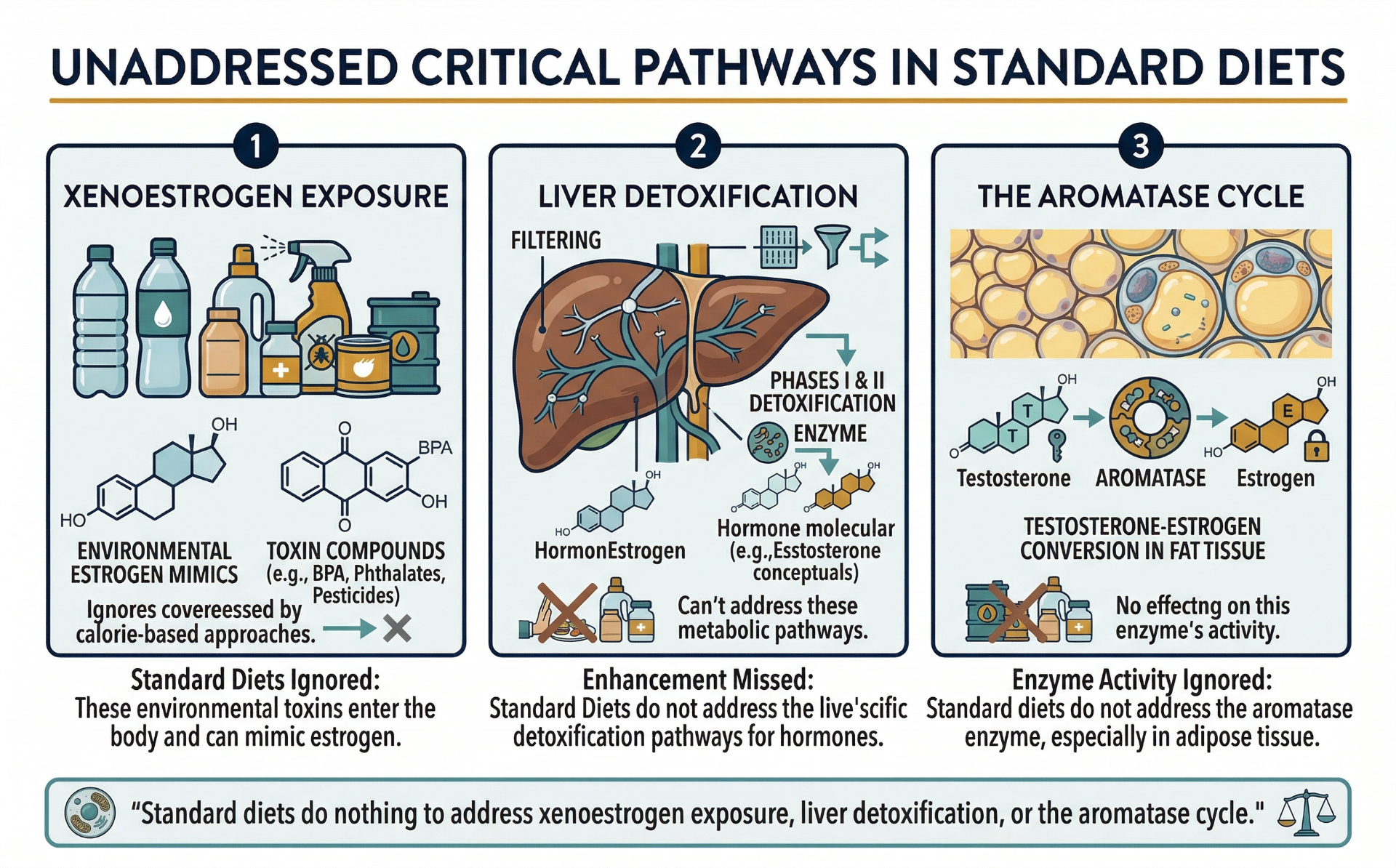
Xenoestrogens. These are environmental compounds that mimic estrogen activity at the receptor level ¹³. The most studied include bisphenol A (BPA) found in plastics and thermal receipts, phthalates in personal care products, and certain pesticides. The cumulative load from modern environments is significant and was simply not present at this scale a generation ago ¹⁴.
Liver burden. Anything that taxes the liver, including alcohol, certain medications, processed food, and environmental toxins, can divert capacity away from estrogen clearance ¹⁵.
Gut dysbiosis. Modern diets, antibiotic exposure, and chronic stress disrupt the estrobolome, leading to enhanced beta-glucuronidase activity and estrogen recirculation ¹⁶.
Methylation impairment. Variations in the MTHFR gene, low folate or B12 intake, or alcohol consumption can reduce methylation capacity, slowing the most important Phase 2 pathway ¹⁷.
Adipose accumulation. As mentioned, fat tissue is hormonally active. The more adipose tissue, the more aromatase activity, the more endogenous estrogen production ¹⁸.
Chronic stress. Cortisol elevation diverts hormonal precursors away from progesterone production (sometimes described as the ‘pregnenolone steal’) ¹⁹, reducing the progesterone that would otherwise balance estrogen activity.
Perimenopause. The hormonal volatility of perimenopause can create relative estrogen dominance in many women, sometimes for years before menopause itself ²⁰.
The High Estrogen pattern is one of the more clearly self-reinforcing of the five Hormetics types. The mechanism is direct:
For both women and men, this pattern can persist for years and is often resistant to standard dietary approaches because the standard approaches do not address the clearance side of the equation.

Most of the popular discussion around estrogen tends to focus on either production or replacement: lower the estrogen, or supplement it during menopause. Both can be appropriate clinically. Neither, on its own, addresses the clearance pathway.
For women, the standard approach to symptoms in the perimenopausal years is often hormonal contraception or hormone replacement therapy, which can be valuable but does not address the underlying detoxification capacity ²¹. For men, the popular discussion of testosterone has expanded considerably, but the relationship between testosterone and estrogen (mediated by aromatase activity in fat tissue) is less commonly addressed ²².
For both sexes, standard dietary interventions often produce frustrating results in this pattern because the issue is not calorie balance but tissue-specific fat retention. Cellulite, lower body adiposity, and chest tissue changes are particularly resistant to standard caloric approaches because they are hormonally rather than calorically driven ²³.
The deeper limitation is that conventional approaches tend to treat estrogen as a single number to be raised or lowered, rather than as a system involving production, balance, clearance, and recirculation.
The High Estrogen framework starts from the recognition that the body's ability to process and eliminate estrogen is at least as important as its production.
This is what the Hormetics system addresses for this type. The Estrogen Reset Protocol, co-developed by Elwin Robinson and Dr. Miriam Mikicki MD, works through the clearance pathways in a specific order. The details of the protocol are beyond the scope of this page, but the framework addresses liver detoxification capacity, gut estrobolome health, environmental xenoestrogen exposure, methylation support, and lifestyle factors that influence aromatase activity. The approach is the same regardless of sex, though the emphasis varies. Both women and men can present with this pattern, and the underlying mechanisms are largely the same.
The first step is identifying which of the five Hormetics types applies to your specific situation.
The High Estrogen pattern frequently overlaps with other Hormetics types. It commonly co-presents with leptin resistance because adipose tissue produces both leptin and estrogen ²⁴. It often appears alongside cortisol dominance because chronic stress reduces progesterone, leaving estrogen relatively unopposed ²⁵. Insulin resistance compounds the pattern by upregulating aromatase activity.
If the description on this page sounds like your experience, the next step is the Hormetics Assessment.
Already taken the assessment and know you're a Estrogen Type? If so, the following could help:
What to eat, what to avoid, the supplements that support the pattern, and the daily rhythms that move the needle on healthy estrogen metabolism.
Learn More
Formulated to support healthy estrogen metabolism and hormonal balance.†
Learn MoreImportant: The Hormetics framework is an educational system designed to support hormonal and metabolic optimization. It is not a substitute for medical evaluation, diagnosis, or treatment. If you have a medical condition, are taking medication, or have specific health concerns, consult with your healthcare provider before making changes. Individual results vary.
We use cookies to ensure the best experience and for ad performance.