The Insulin Reset Protocol
The complete protocol for the insulin type — meal structure that brings insulin back to baseline, the foods to prioritise, and the daily rhythms that get blood sugar working with you instead of against you.
Learn MoreWhen your blood sugar test is normal but your body is telling a different story
The afternoon crash. The 3 PM brain fog. The midsection weight that will not move no matter how clean the diet. The doctor's lab work that comes back ‘normal’ but does not match how you feel. There is a reason these things show up together.
The High Insulin Type is the second of the five hormonal patterns identified in the Hormetics framework, co-developed by health researcher Elwin Robinson and Dr. Miriam Mikicki MD, an IFM-certified functional medicine physician.
If you have noticed any of the following, insulin signaling may be a meaningful part of your situation:
These are signs commonly associated with insulin resistance, a pattern that develops gradually over years before it ever shows up on a routine blood glucose test ¹.
Insulin is one of the most important regulatory hormones in the human body. It is produced by the beta cells of the pancreas in response to rising blood glucose, primarily after meals ². Its main job is to act as a key, opening cellular receptors so that glucose, amino acids, and fatty acids can move out of the bloodstream and into the cells that need them ³.
Beyond that, insulin is a master regulator of fuel storage. When insulin is high, the body is in a fed and storing state. When insulin is low (between meals, during sleep, after fasting), the body is in a fasted and burning state. The healthy oscillation between these two states is the foundation of metabolic flexibility ⁴.
This is what insulin is supposed to do.
Insulin resistance is the gradual loss of cellular sensitivity to insulin. The pancreas keeps producing insulin in response to meals. The cells stop opening their doors as readily. To compensate, the pancreas produces more insulin, then more, then more again ⁵.
This is the part that conventional testing tends to miss.
Standard blood sugar testing measures glucose, not insulin. In the early stages of insulin resistance, glucose levels often remain in the normal range because the pancreas is working overtime to keep them there ⁶. The cost (hyperinsulinemia, chronically elevated insulin) does not show up unless someone specifically tests fasting insulin or runs a HOMA-IR calculation ⁷.
This means the pattern can develop for five, ten, even fifteen years before it triggers a ‘diabetic’ or ‘pre-diabetic’ diagnosis ⁸. By that point, the pancreas is exhausted, glucose has finally risen, and the standard interventions begin. But the underlying issue (the cellular insensitivity) has been driving symptoms the entire time.
Joseph Kraft, a pathologist who tested the post-meal insulin response of more than 14,000 patients over several decades, found that elevated insulin nearly always preceded elevated glucose, often by a decade or more ⁹. His work suggests that insulin resistance is far more common than glucose-only testing reveals.
The drivers of insulin resistance are well established in the research and concentrate on a small number of root causes.
Refined carbohydrate exposure. Foods that trigger sharp glucose elevations require correspondingly sharp insulin responses. Repeated daily, this trains the system toward chronic hyperinsulinemia ¹⁰. White flour, refined sugar, fruit juice, and processed snack foods are the most concentrated sources.
Snacking patterns. Insulin levels do not return to baseline as long as food keeps arriving. Modern eating patterns (three meals plus several snacks daily) keep insulin elevated for most waking hours, denying cells the recovery period they need ¹¹. This is one of the most underappreciated drivers in the literature.
Visceral fat accumulation. Fat stored around the organs (rather than under the skin) is metabolically active and directly contributes to insulin resistance through inflammatory cytokine production ¹².
Sleep deprivation. Even a single night of restricted sleep measurably reduces insulin sensitivity in healthy individuals ¹³. Chronic sleep loss is consistently associated with elevated fasting insulin and HOMA-IR ¹⁴.
Sedentary lifestyle. Skeletal muscle is the largest insulin-sensitive tissue in the body. When muscles are not contracted regularly, their insulin sensitivity declines ¹⁵. Even brief post-meal walking has been shown to meaningfully blunt the insulin response ¹⁶.
Specific food triggers. Industrial seed oils and trans fats have been associated with worse insulin sensitivity in multiple studies ¹⁷. Coffee on an empty stomach has been shown to acutely impair glucose tolerance in some individuals ¹⁸.
Insulin resistance is a self-reinforcing pattern. As cells become less responsive to insulin, the pancreas produces more. As insulin levels rise, fat storage is favored over fat burning. As fat (particularly visceral fat) accumulates, inflammatory signals worsen insulin sensitivity further. As sensitivity worsens, more insulin is required. And so on ¹⁹.
The downstream consequences extend well beyond weight. Hyperinsulinemia is associated with elevated blood pressure ²⁰, dyslipidemia ²¹, increased cardiovascular risk ²², cognitive concerns ²³, and the cluster of conditions known as metabolic syndrome.
It is also a major contributor to cravings. Insulin's interaction with the satiety system, including its overlap with leptin signaling, means that high insulin states often coexist with disordered appetite ²⁴. People with insulin resistance frequently describe feeling hungry on a schedule, regardless of whether they have actually eaten enough.
The standard advice for blood sugar concerns tends to focus on glucose, not insulin. This makes sense when treating diagnosed diabetes, but it can mask insulin resistance for years.
Two common approaches deserve specific mention.
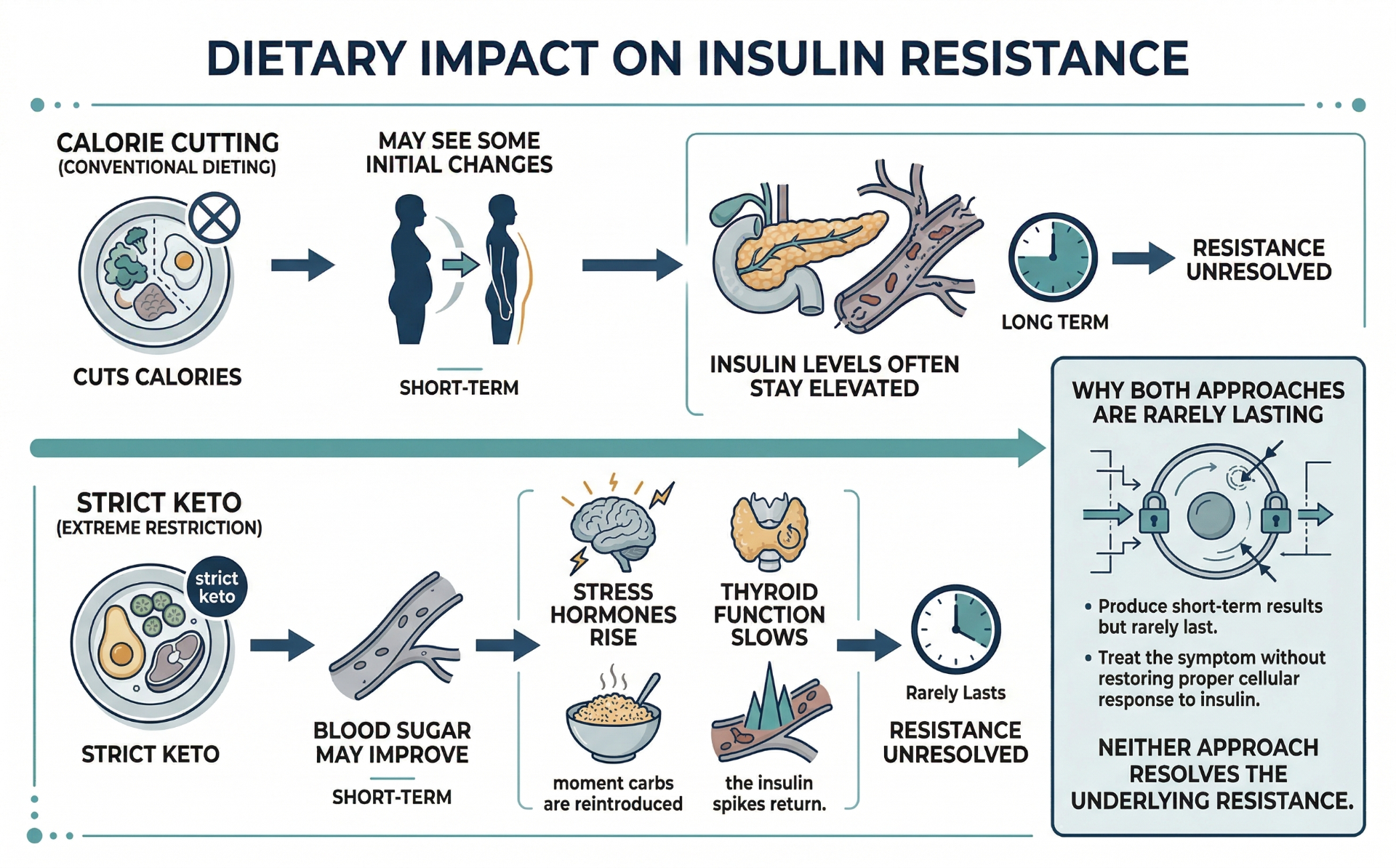
Calorie-restricted, low-fat diets. These were the standard recommendation for metabolic concerns for several decades. The problem is that they often replace fat calories with refined carbohydrates, which can worsen insulin response ²⁵. These protocols often produce initial body composition changes, but insulin resistance frequently persists.
Long-term ketogenic and very-low-carb approaches. These can produce striking short-term improvements in insulin sensitivity by directly reducing the carbohydrate load ²⁶. The concern in the longer-term literature is that very strict ketogenic protocols can elevate cortisol ²⁷, reduce thyroid output ²⁸, and produce a metabolic slowdown that creates new problems. The Hormetics view, supported by Dr. Mikicki's clinical observations, is that moderate carbohydrate intake combined with proper meal timing tends to be more sustainable than chronic restriction.
Both approaches share a deeper limitation: they treat the input (carbohydrates) without addressing the upstream context (chronic snacking, poor sleep, sedentary patterns) that allows insulin resistance to develop in the first place.
The High Insulin Type framework starts by reframing the problem: insulin resistance is not about how much glucose you ate at one meal, but about the cumulative pattern of insulin elevation across days, weeks, and years.
This is what the Hormetics system addresses for this type. The Insulin Reset Protocol, co-developed by Elwin Robinson and Dr. Miriam Mikicki MD, works through the structural drivers of chronic hyperinsulinemia rather than focusing exclusively on macronutrient ratios. The specifics of the protocol are beyond the scope of this page, but the framework addresses meal timing and structure, food quality, post-meal physical activity, sleep optimization, and targeted nutritional support. It does not require ketogenic restriction, prolonged fasting, or any approach that would be unsustainable as a long-term way of eating.
The first step is identifying which of the five Hormetics types applies to your specific situation.
The High Insulin pattern frequently overlaps with other Hormetics types. Insulin resistance and leptin resistance share common inflammatory drivers and often appear together ²⁹. Cortisol elevation directly promotes insulin resistance through hepatic gluconeogenesis ³⁰. Estrogen imbalance can also affect insulin sensitivity in both men and women ³¹.
This is why a single-mechanism approach often falls short for the people most affected.
If the description on this page sounds like your experience, the next step is the Hormetics Assessment. It will tell you whether insulin signaling is your dominant pattern, a secondary factor, or not applicable to your situation.
Already taken the assessment and know you're a Insulin Type? If so, the following could help:
The complete protocol for the insulin type — meal structure that brings insulin back to baseline, the foods to prioritise, and the daily rhythms that get blood sugar working with you instead of against you.
Learn More
Formulated to support healthy blood sugar balance and metabolic function.†
Learn MoreImportant: The Hormetics framework is an educational system designed to support hormonal and metabolic optimization. It is not a substitute for medical evaluation, diagnosis, or treatment. If you have a medical condition, are taking medication, or have specific health concerns, consult with your healthcare provider before making changes. Individual results vary.
We use cookies to ensure the best experience and for ad performance.