The Leptin Reset Protocol
The complete protocol for the leptin type — how to restore proper satiety signals, the foods that work with your hunger hormones instead of against them, and the daily rhythms that bring leptin sensitivity back.
Learn MoreWhen the satiety signal stops getting through
You finish a full meal. The plate is clean. Your stomach is physically full. But twenty minutes later, you are already thinking about what to eat next. That has a name. It is not a discipline issue. And it is not something you imagined.
The High Leptin Type is one of the five hormonal patterns identified in the Hormetics framework, co-developed by health researcher Elwin Robinson and Dr. Miriam Mikicki MD, an IFM-certified functional medicine physician.
If you have noticed any of the following over time, you may be looking at a leptin signaling pattern:
The more of these patterns line up with your experience, the more likely leptin signaling is part of the picture. The good news is that this pattern is well documented in the scientific literature ¹, and the mechanisms behind it are increasingly well understood.
Leptin is a hormone discovered in 1994 ². It is produced primarily by fat cells, and its main job is to communicate with the brain. Specifically, it talks to a region called the hypothalamus, which sits at the base of the brain and acts as the central regulator of appetite, energy expenditure, and metabolism ³.
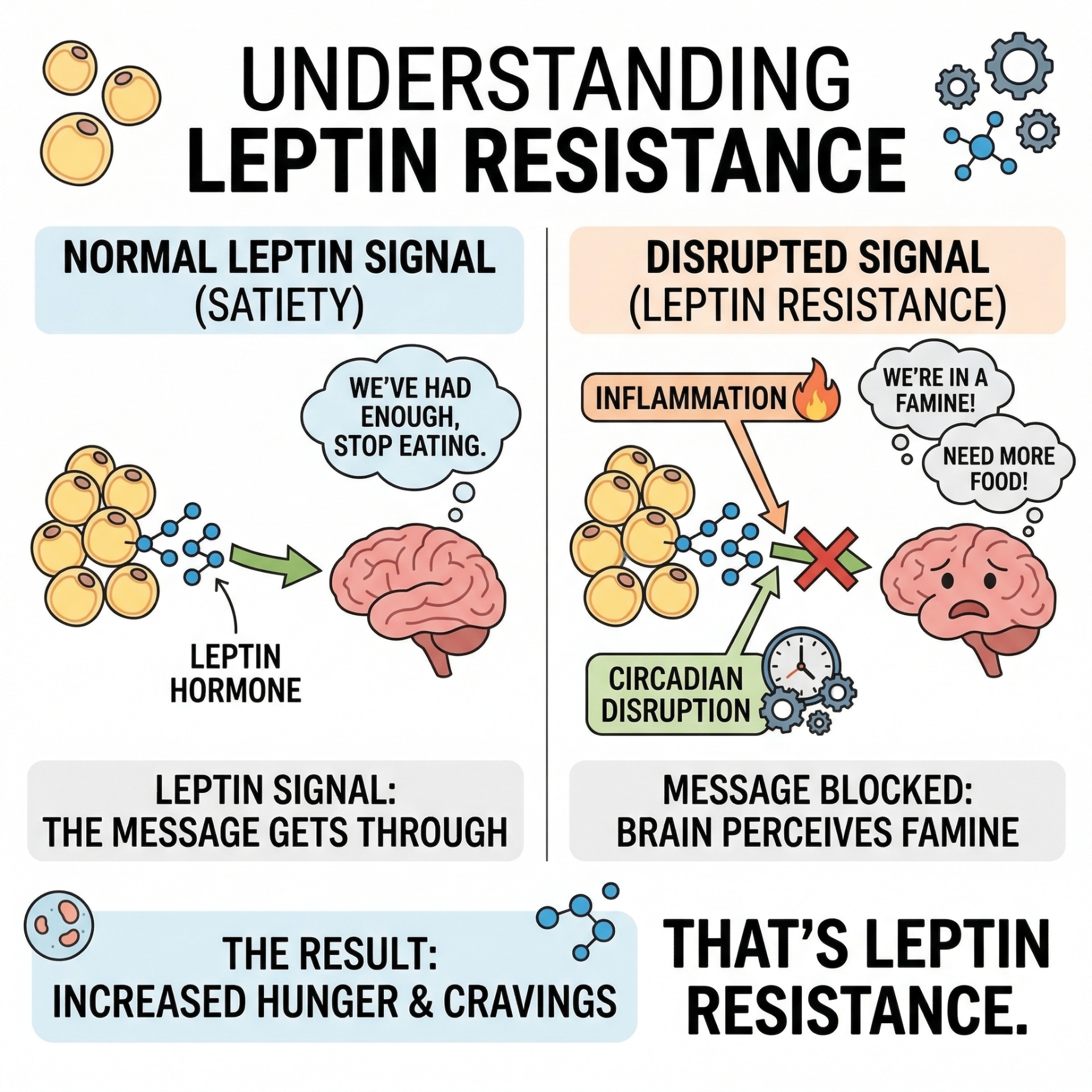
The simplest way to think about leptin is as a status report. The body uses it to send the brain a continuous signal that says, in effect: we have enough energy stored, you can stop eating. When leptin levels rise, appetite is supposed to fall. When energy reserves drop, leptin falls, and appetite rises. That is how the system is meant to work ⁴.
In a healthy signaling environment, this loop is exquisitely sensitive. The brain integrates the leptin signal with other inputs (insulin, ghrelin, glucose levels, stomach distension) and produces the experience of being satiated, which is the feeling of being genuinely done with a meal. Satiation is not the same as fullness. Fullness is mechanical, the stomach being physically expanded. Satiation is neurological, the brain registering that the body has what it needs ⁵.
This distinction matters. People with the High Leptin pattern often report that they can feel physically full but not satiated. The plate is empty. The stomach is stretched. But the brain is still asking for more.
Here is the strange paradox at the heart of leptin resistance: people with this pattern usually have more leptin in their blood than other people, not less ⁶. As body fat increases, fat cells produce more and more leptin, trying to amplify the signal. Yet the brain becomes progressively less responsive to it.
This is the resistance. Not a deficiency.
Why does the brain stop listening? The most well-supported explanation in the research literature points to inflammation, specifically inflammation in the hypothalamus itself ⁷. When the hypothalamic neurons that detect leptin become inflamed, the receptors and downstream signaling molecules stop functioning properly. The leptin keeps arriving. The receptor cannot transduce the signal. The message never reaches the parts of the brain that produce the feeling of 'enough.'
Several specific molecular pathways have been implicated:
The practical translation: when the hypothalamus is inflamed, no amount of additional leptin solves the problem. This is why early attempts to treat the condition by giving people exogenous leptin produced disappointing results ¹². The problem was never a shortage of the hormone. The problem was a receiver that was no longer tuned to it.
Leptin signaling does not break overnight. It typically develops over months and years through repeated exposure to a small number of upstream drivers. The research has converged on several main contributors.
Chronic inflammation. Whatever the source, persistent low-grade inflammation appears to be the central upstream driver. This includes inflammation from processed foods (particularly industrially refined seed oils and high-fructose corn syrup) ¹³, from chronic stress ¹⁴, from poor sleep ¹⁵, from gut dysbiosis ¹⁶, and from environmental toxin exposure ¹⁷.
Sleep disruption. Leptin signaling is tightly linked to circadian biology. Sleep deprivation directly suppresses leptin and elevates ghrelin, the opposing appetite hormone, even with no change in diet ¹⁸. Across decades of human studies, restricted sleep correlates with increased calorie intake the following day ¹⁹.
Light environment. Bright morning light and dim evening light help anchor the circadian rhythms that regulate leptin sensitivity ²⁰. Modern indoor environments, with their inverted light patterns (dim mornings, bright nighttime screens), disrupt these rhythms.
Refined fructose. A specific concern in the leptin literature, separate from sugar intake generally. Refined fructose has been shown to interfere with leptin transport across the blood-brain barrier ²¹ and to drive hepatic insulin resistance, which compounds the problem ²².
Chronic psychological stress. Cortisol elevation promotes inflammation and disrupts the hormonal milieu in which leptin operates ²³.
For most people with this pattern, the situation is some combination of these factors, accumulated over time, rather than any one cause in isolation.
One reason this pattern is so persistent is that it tends to compound on itself. As leptin resistance develops, the brain interprets the missing satiety signal as evidence of a famine. It responds by doing exactly what it would do in a real famine: increasing hunger, lowering energy expenditure, conserving fuel ²⁴.
This means a person with leptin resistance is fighting two systems at once. The first is the broken signal itself, which keeps them eating past genuine need. The second is the body's starvation response, which makes calorie restriction not just unpleasant but biologically punishing. Studies of post-diet rebound consistently show that the body defends against energy deficit with persistent hormonal counter-regulation, sometimes for years afterward ²⁵.
The result is a feedback loop that does not break on its own:
This is why people with this pattern so often describe feeling like their body is working against them. In a sense, it is.

The standard advice for someone struggling with appetite is some version of 'eat less, move more.' For the High Leptin pattern, this advice can actually make the underlying problem worse.
When the brain is already misreading the body's energy state as deficient, dropping calories deepens the misread. The starvation response intensifies. Hunger gets sharper. Metabolic rate slows further ²⁶. The body becomes more efficient at storing what little comes in. And when the diet inevitably ends, the rebound is often greater than the loss.
GLP-1 medications take a different approach. They mechanically slow stomach emptying and produce a sense of fullness regardless of the leptin signal ²⁷. For some people, this is genuinely useful. But it does not address the underlying inflammation, the receptor sensitivity, or the upstream drivers. As Elwin Robinson has put it: 'I would far rather work on the leptin level than the GLP-1 level, at least initially.' Dr. Mikicki agrees that medications can be appropriate in specific clinical situations, particularly when lifestyle approaches have not yet been engaged with.
The deeper issue is that calorie-focused approaches treat the symptom (eating too much) rather than the signal (the brain not registering 'enough'). Until the signal is restored, the appetite is going to keep showing up.
The High Leptin Type framework starts from a different question: what is interfering with the satiety signal in this specific pattern, and what can be done to restore it?
This is what the Hormetics system addresses. Co-developed by Elwin Robinson and Dr. Miriam Mikicki MD, the system identifies five hormonal patterns that influence metabolism and body composition, with leptin being one of them. For people who fit the High Leptin pattern, there is a structured framework called the Leptin Reset Protocol, which works through the upstream drivers in a specific order. The details of the protocol are beyond the scope of this page, but the framework targets the inflammation, sleep, light environment, stress signaling, and nutritional factors that underlie the resistance pattern in the first place.
The first step is identifying which of the five Hormetics types applies to your situation. Some people are clearly one type. Many are a combination. The Hormetics Assessment is a free 80-question diagnostic that maps your specific pattern.
It is worth mentioning that the High Leptin pattern rarely shows up alone. Leptin resistance and insulin resistance often co-occur because the inflammatory drivers overlap ²⁸. Estrogen dominance can amplify leptin production because adipose tissue produces both ²⁹. Cortisol elevation promotes the hypothalamic inflammation that sits underneath all of these patterns ³⁰.
This is why a single-mechanism approach (just reducing calories, just adding a supplement, just treating one hormone) often falls short for the people most affected. Bodies are systems. Hormones interact. The Hormetics framework is built around this reality.
If the description on this page sounds like your experience, the next step is the assessment. It will tell you whether leptin signaling is your dominant pattern, a secondary factor, or not applicable to your situation, along with what other patterns may be in play.
Already taken the assessment and know you're a Leptin Type? If so, the following could help:
The complete protocol for the leptin type — how to restore proper satiety signals, the foods that work with your hunger hormones instead of against them, and the daily rhythms that bring leptin sensitivity back.
Learn More
A targeted blend of African Mango Seed, Ceylon Cinnamon, and Alpha-Lipoic Acid — formulated to support healthy appetite regulation, leptin sensitivity, and the body’s natural satiety signals throughout the day.†
Learn MoreImportant: The Hormetics framework is an educational system designed to support hormonal and metabolic optimization. It is not a substitute for medical evaluation, diagnosis, or treatment. If you have a medical condition, are taking medication, or have specific health concerns, consult with your healthcare provider before making changes. Individual results vary.
We use cookies to ensure the best experience and for ad performance.