The Metabolism Reset Protocol
The eat-more-to-feel-better framework, the foods that signal safety to the body, and the daily rhythms that shift you out of hibernation mode.
Learn MoreWhen eating less makes things harder, not easier
You eat less than the people around you and you are still gaining weight or holding onto it. You are cold. You are tired. Your hair, your nails, your skin, all of them have lost some quality you remember having. Your thyroid tests come back ‘normal.’ But something is off. There is a name for this pattern.
The Low Metabolism Type is the fifth of the five hormonal patterns in the Hormetics framework, co-developed by health researcher Elwin Robinson and Dr. Miriam Mikicki MD, an IFM-certified functional medicine physician.
If the following picture is recognizable, low metabolism may be a meaningful part of your situation:
The defining feature of this pattern is that the conventional advice (eat less, move more) tends to make the underlying problem worse, not better ¹.
Metabolism is the rate at which the body produces and uses energy. At the cellular level, it is the work done by mitochondria, small organelles inside every cell that convert nutrients (glucose, fat, ketones) into a molecule called ATP, the universal energy currency of the body ².
Two main inputs control how fast the mitochondria run:
Substrate. The cells need fuel (glucose, fatty acids) and the cofactors that turn them into ATP (B vitamins, magnesium, iron, CoQ10, and others) ³.
Signal. The cells need a hormonal signal to run faster or slower. The primary signal is thyroid hormone. Specifically, the active form, T3 (triiodothyronine), binds to receptors in nearly every cell of the body and increases mitochondrial activity, oxygen consumption, and heat production ⁴.
The thyroid gland produces mostly T4 (the inactive storage form), which then needs to be converted to T3 in peripheral tissues, particularly the liver, kidneys, and gut ⁵. This conversion step is critical and is one of the most common bottlenecks in the metabolic system.
A healthy metabolic system has adequate fuel, adequate cofactors, and adequate T3 reaching the cells. When any of these is impaired, energy production drops and the metabolic rate falls.
Low metabolism, in most cases, is not a thyroid disease in the conventional sense. Most people with this pattern have technically normal TSH levels (the standard screening test) and would not be diagnosed with hypothyroidism by their primary care physician ⁶.
What is happening instead is more subtle. The thyroid is producing T4, but the conversion to T3 is impaired. Or T3 is being converted to its mirror-image inactive form, called reverse T3 (rT3), which occupies receptors without activating them ⁷. Or the mitochondria themselves are dysfunctional, even when the thyroid signal is intact.
Several specific mechanisms are well-documented in the research:
Famously, follow-up research on contestants from ‘The Biggest Loser’ found that years after the show, their resting metabolic rate remained hundreds of calories per day below predicted levels, with persistent reductions in thyroid output ¹⁴. This study, while specific in its population, illustrates a general phenomenon: the metabolism does not necessarily reset when the diet ends.
The drivers of low metabolism cluster around a small number of common origins.
Chronic dieting. Repeated cycles of caloric restriction are arguably the most common entry point. Each round teaches the body that calories are scarce and signals adaptation downward ¹⁵.
Prolonged ketogenic or very-low-carb eating. Carbohydrates are an important substrate for T4 to T3 conversion. Sustained low-carb intake can suppress conversion in some individuals ¹⁶.
Excessive endurance exercise. Long-duration cardio without adequate fuel or recovery is associated with reduced thyroid output and elevated cortisol ¹⁷.
Iodine deficiency. Despite iodized salt, modern diets often fall short of optimal iodine intake ¹⁸.
Industrial seed oil exposure. Polyunsaturated fatty acids from refined seed oils can affect mitochondrial membrane function over time ¹⁹.
Environmental toxin load. Heavy metals, certain plastics, and halogen exposure (fluoride, bromide) can interfere with iodine uptake and thyroid function ²⁰.
Chronic infections. Persistent low-grade infections suppress thyroid function as part of the body's energy conservation response ²¹.
Aging. Mitochondrial efficiency decreases with age, contributing to a gradual metabolic decline that is normal but can be optimized ²².
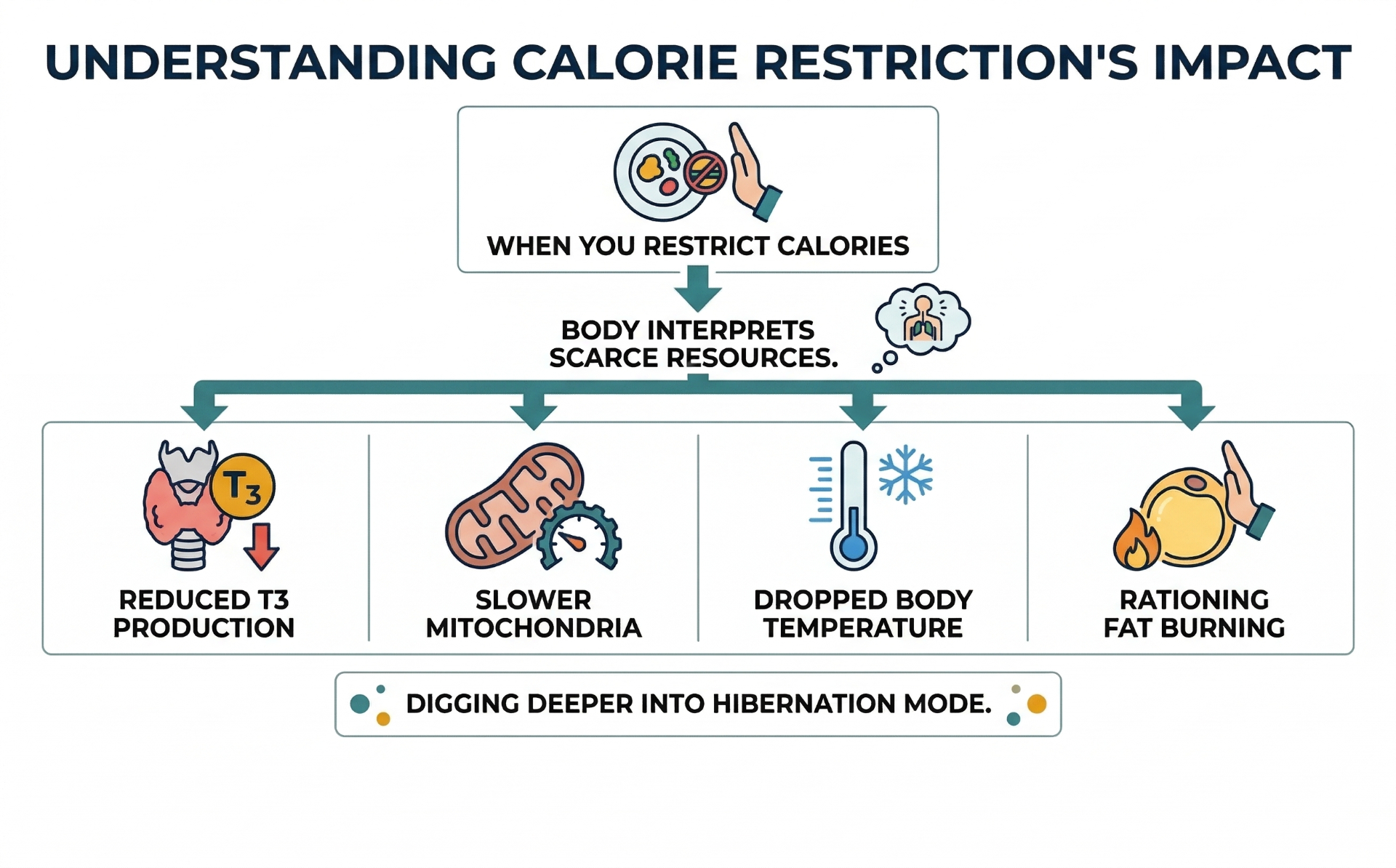
The Low Metabolism pattern is particularly insidious because the standard interventions (eat less, exercise more) tend to deepen the underlying problem. The cycle works as follows:
This is the classic pattern documented across the metabolic adaptation literature ²³. The person's effort is intensifying while their results are worsening.
The conventional approach to slow metabolism has two main forms.
Standard medical screening with TSH only. This catches the most severe cases of hypothyroidism but misses most of the functional patterns described above ²⁴. A TSH in the upper-normal range, combined with low T3 and elevated rT3, can produce significant symptoms while still being labeled normal. A growing body of clinical literature argues for routine assessment of free T3 and reverse T3 alongside TSH ²⁵.
The standard prescription. Eat less and exercise more. For this specific type, this often deepens the pattern. The body responds to caloric scarcity by slowing metabolism further as an adaptive response ²⁶.
A third common intervention, thyroid medication (typically synthetic T4), can be appropriate in clear cases of hypothyroidism. But for the common functional patterns (normal TSH with low conversion or mitochondrial issues), T4 alone is often insufficient because the bottleneck is at the conversion step rather than at production ²⁷.
The deeper limitation of conventional approaches is that they tend to treat metabolism as a fixed property of the person rather than as a dynamic system that responds to inputs.
The Low Metabolism Type framework starts from a different premise: the metabolic rate is highly responsive to inputs, but the inputs are usually not the ones the standard advice focuses on.
This is what the Hormetics system addresses for this type. The Metabolism Reset Protocol, co-developed by Elwin Robinson and Dr. Miriam Mikicki MD, works through the structural drivers of suppressed metabolism in a specific order. The details of the protocol are beyond the scope of this page, but the framework addresses thyroid substrate (the nutrients required for T3 production), the drivers of reverse T3, mitochondrial function, light and stress signaling, and adequate fuel intake to signal metabolic safety. The approach is counterintuitive for most people because it does not start with restriction. It starts with signaling the body that there is no famine.
In Elwin's words: ‘When your metabolism starts speeding up, everything starts speeding up, and then suddenly your body's like, oh, we can deal with all that stuff now. We're not in hibernation mode anymore.’
Low Metabolism rarely operates in isolation. It frequently develops as a downstream consequence of cortisol dominance (which inhibits T3 conversion) ²⁸, leptin resistance (where the body has been signaling perceived starvation for years) ²⁹, and chronic inflammatory states from any source ³⁰. It can also accompany estrogen dominance through the impact of estrogens on thyroid binding globulin ³¹.
This is why a single-mechanism approach, especially one focused only on the thyroid itself, often falls short.
If the description on this page sounds like your experience, the next step is the assessment.
Already taken the assessment and know you're a Low Metabolism Type? If so, the following could help:
The eat-more-to-feel-better framework, the foods that signal safety to the body, and the daily rhythms that shift you out of hibernation mode.
Learn More
Formulated to support healthy thyroid function, mitochondrial energy production, and cellular metabolism.†
Learn MoreImportant: The Hormetics framework is an educational system designed to support hormonal and metabolic optimization. It is not a substitute for medical evaluation, diagnosis, or treatment. If you have a medical condition, are taking medication, or have specific health concerns, consult with your healthcare provider before making changes. Individual results vary.
We use cookies to ensure the best experience and for ad performance.